Soon after I published Food As Medicine in 2011, I received an email from a reader, who wrote about her experience with migraines and magnesium. A long-time lacto-ovo vegetarian, she told me that she took supplemental magnesium each month to control her premenstrual migraines, and that it was the only thing that worked for her.
To be sure, it’s been known for years that magnesium can be helpful in the prevention of premenstrual migraines. Several studies have shown that low serum magnesium is an independent risk factor for migraine headaches, and that magnesium can be used therapeutically to both prevent and treat migraines, as well as a host of other disorders characterized by spasm.
She couldn’t understand why she might be magnesium-deficient, however, because she ate a lot of brown rice, and had been told that brown rice was high in magnesium. According to nutritiondata.com, rice indeed tops the list of all magnesium-containing foods, at 781 mg per 100 mg. Although this refers specifically to just the bran and not the whole grain cereal itself, brown rice still weighs in at a respectable 143 mg of magnesium per 100 g serving. Thus if she ate about three cups of cooked brown rice (about 550 g) on a daily basis, she should have been getting more than 780 mg of magnesium, which is a significant dose by any standard.

It was only after this woman read the sections in Food As Medicine that discuss the importance of fermenting cereals to enhance nutrient absorption, that she put two and two together. Following the instructions in the book (see below), she began to ferment her brown rice before cooking, and a few weeks later noticed that she didn’t experience the same intensity of premenstrual migraines. Inspired by her results, she continued to practice this technique for the next two months, reporting to me in her email that her migraine issues were apparently resolved. Any of my students enrolled in my Food As Medicine program won’t find this to be much of a surprise. One of the central tenets of my nutritional approach is that our issue with diet and its disease-causing potential is a direct result of industrial technologies supplanting traditional methods of food preparation.
All seeds (or more properly ‘fruits’), whether they be cereals, legumes, nuts, or what conventionally call “seeds”, contain a host of natural plant chemicals that serve to discourage predation by animals. This is done to ensure reproductive success, and while this strategy isn’t necessarily effective against all predators, such as insects and birds, it has been very successful against mammalian predators. The extensive grasslands found all over the world are a testament to just how effectively grass seed resists mammalian digestion, and how the grass actually uses these predators to spread it further afield. Such is the strategy of many plants, that sacrifice a part of themselves to ensure the distribution of their genetic material, hopefully dispersed intact, contained within a nutrient-dense clump of “fertilizer”.

Among mammals, however, humans are unique for our relatively recent practice of consuming cereal and legume crops as staples. While a variety of seeds have long been a part of the human diet, the proportion consumed for pre-agrarian peoples was much lower when compared to the farming folk that began to emerge during the 9-10th millennia BCE. The archeological record shows that in every measurable way human health declined with this transition, with clear evidence of physical degeneration, including a loss of height and bone density, and a dramatic increase in dental and skeletal problems.
While this issue of diet and physical degeneration remains perennial throughout the history of human agriculture, the problem stabilizes and begins to reverse as early farming societies discovered the importance of using food preparation techniques such as fermentation, to increase digestibility and nutrient absorption. Since this time, traditional agricultural societies have maintained an unbroken practice of using such techniques to process cereals and legumes, and optimize health. Besides the traditional sourdough breads of Europe, examples of this can be seen all over the world, in traditional foods such as chocolate (from cacao, Central America), ogi (from sorghum, West Africa), injera (from teff, East Africa; pictured below), idli (from rice and urad, South India), and natto (from soy, Japan).

As I articulated earlier, the global exportation of industrial food technologies has meant that much of this knowledge is rapidly disappearing or has been lost entirely. In all of the regions I mention above, industry has either begun to or has entirely supplanted these traditions, as it has in Westernized, ‘First-world’ nations. As a result, we can see how Westernized patterns of disease have crept into these societies, to promote an increasing prevalence of digestive, cardiometabolic, and autoimmune disease. Billions and billions of research dollars are spent each year trying to find a cure for these diseases, when in many cases the cause is entirely related to a loss of traditional knowledge and practices. In 2011, I made the point in Food As Medicine that when wheat is properly fermented, it no longer elicits an immunological reaction in patients diagnosed with celiac disease. This demonstrates that the cause of celiac disease is directly related to a failure to maintain traditional food practices. In my opinion, this finding is just the tip of the iceberg in a huge range of digestive and inflammatory disorders that could otherwise be prevented.
Of course this epiphany for the most part continues to elude modern science, which due to monied interests and its myopic pursuit speculative, novel solutions, has little time for moldy old traditions like food fermentation. But in my clinical experience, and as demonstrated by this woman’s experience with brown rice, we continue to ignore traditional wisdom at the peril of chronic disease.
In Food As Medicine, I discuss two basic methods to ferment cereals and legumes. One way to prepare them is to half-cook them first, and then ferment them in a brine, using some leftover live-culture pickle juice as an inoculant. The last part of the following video (start at 4:47) describes the technique for fermenting cooked chickpeas:
While this makes for a very satisfying result, especially for making bean dishes like hummus, it does take several weeks before its ready. Another technique I mention is a pre-cooking fermentation method, that once you’ve got an inoculum going, only takes 24 hours to prepare. Here it is, taken from the book, Food As Medicine:
Fermentation is a key step in ensuring the digestibility of foods such as cereals, legumes, nuts and seeds all of which contain antinutrient factors (ANFs) such as phytic acid and trypsin inhibitors that impair digestion and inhibit the absorption of nutrients. The procedure to ferment these foods begins with making a starter. Soak the nut, seed, grain or legume in water for 24 hours at 86˚F/30˚C, in a ceramic or glass container. If you don’t live in a tropical climate you will need to use something to keep the ferment warm enough, such as an electric heat mat used for sprouting and germinating seeds. After 24 hours, drain off the liquid, but set aside one cup of the soaking water for later use. Rinse the nut, seed, grain or legume, and prepare as normal.
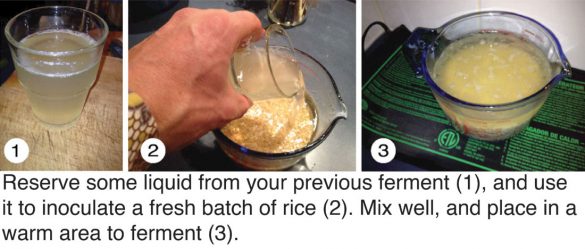
The cup of soaking liquid that you reserved is full of bacteria, and becomes an inoculum (bacterial culture) for the next batch. Repeat the same process with fresh ingredients, but add the inoculum to the soaking water, and let sit at 86˚F/30˚C for 24 hours. After, drain the soaking water and cook as normal, but retain a cup of the soaking water for the next batch. If you keep doing this, by the fourth time you will have an inoculum that is capable of reducing ANFs such as phytic acid by 96%.[1] While fermentation reduces ANFs, however, it does not remove components such as lectins,[1] and thus the nut, seed, grain or legume usually requires additional measures such as cooking.
Once you have created a viable inoculum, you can store it in a covered vessel the refrigerator for up to a week before it will die, but add a handful of brown rice to give it some food.
[1] Liang J, Han BZ, Nout MJR, Hamer RJ. 2008. Effects of soaking, germination and fermentation on phytic acid, total and in vitro soluble zinc in brown rice. Food Chemistry. 110(4): 821-828
[2] Sharma A, Sehgal s. 1992. Effect of processing and cooking on the antinutritional factors of faba bean (Vicia faba). Food Chemistry. 43(5):383-385
So try it out… whether you ferment before or after cooking, doing so will go a long way to improve gut health, and diminish chronic inflammation.





{kind=link}